

Therapy for addiction doesn’t look the way most people imagine it. There’s no leather couch, no silent therapist scribbling notes as you stare at the ceiling. What happens inside these sessions is far more active and more uncomfortable than Hollywood suggests. From the first awkward intake conversation to the raw group discussions that follow, drug addiction treatment unfolds through structured therapeutic work designed to rewire how you think, cope, and respond to the world around you.
If you’ve been putting off treatment because you don’t know what to expect, here’s an honest look at what goes on behind closed doors, and why it works.
What Does the First Session Look Like?
The opening session is less about therapy and more about information gathering. Your therapist needs a complete snapshot before treatment begins – substance history, duration of use, previous attempts at quitting, medical conditions, and mental health symptoms.

Expect a lot of questions. Some feel routine. Others cut deeper than anticipated. You might be asked about childhood experiences, relationship dynamics, or moments when substance use went from recreational to necessary. Each answer helps clinicians identify the triggers, emotional patterns, and co-occurring conditions that shaped your dependency.
Most initial assessments run 60 to 90 minutes. By the end, your treatment team builds a preliminary care plan. They are mapping out which therapy models fit your needs, if medication-assisted treatment makes sense, and how frequently sessions should occur. This blueprint gets revised as therapists learn more about how you respond.
What catches most people off guard is being asked what they want from treatment. Therapists don’t impose goals. They ask you to define what recovery looks like in your own life and work backwards from there.
How Does Individual Therapy Tackle Addictive Patterns?
One-on-one sessions form the backbone of addiction treatment. Sitting across from a therapist with no group buffer feels exposed, and that’s partly the point. Private sessions create space to explore material too personal for a room full of strangers.
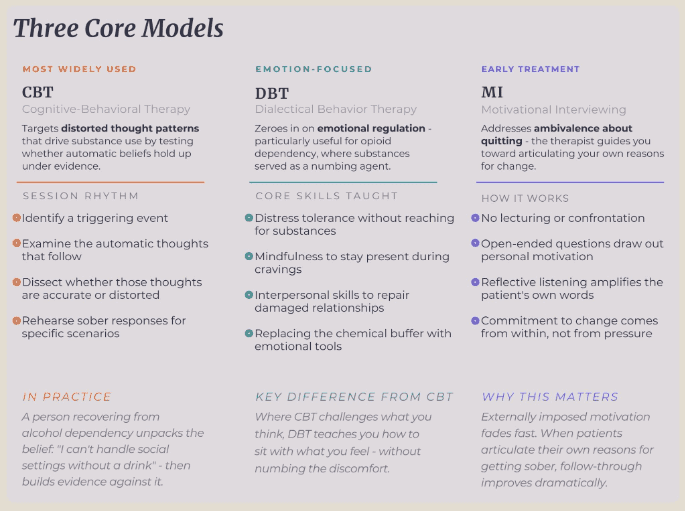
Cognitive-behavioural therapy (CBT) remains the most widely used model. Sessions follow a specific rhythm: identifying a triggering event, examining the automatic thoughts that follow, and dissecting whether those thoughts are accurate or distorted. Through repeated sessions, the therapist helps dismantle that assumption by exploring evidence against it and rehearsing sober responses for specific scenarios.
Dialectical behaviour therapy (DBT) takes a different route. Where CBT targets thought patterns, DBT zeroes in on emotional regulation, particularly useful for opioid dependency, where substances served as a numbing agent. Sessions teach distress tolerance, mindfulness, and interpersonal skills that replace the chemical buffer patients relied on for years.
Motivational interviewing (MI) is most evident in early treatment, when ambivalence about quitting is high. The therapist doesn’t lecture. They guide you toward articulating your own reasons for change, a technique that proves far more effective than external pressure.
Why Do Group Sessions Create Breakthroughs Most People Don’t Expect?
Walking into your first group therapy session feels like the last place you want to be. But something loosens once the conversation starts moving.
Groups gather 6 to 12 participants led by one or two trained counsellors. Some are open-ended, where members discuss whatever surfaces. Others are psychoeducational, built around specific themes like relapse triggers or anger management.
The real power isn’t in the curriculum. It’s in the mirror effect. Hearing someone describe the exact spiral you’ve been living through the lies, the isolation, the bargaining creates a recognition that no individual session can replicate. Shame loses its grip when you realize you aren’t uniquely broken.
Accountability plays a role, too. Group members track each other’s growth and call out avoidance behaviours with the kind of directness therapists sometimes can’t match. Peer confrontation, when it comes from someone who’s walked the same path, lands differently than clinical feedback.

Relapse prevention groups deserve special mention. These sessions equip participants with concrete skills: identifying high-risk environments, creating emergency action plans, and practicing refusal techniques through role-play.
How Do Therapy Techniques Change Depending on the Substance?
Not all addictions respond to the same therapeutic model. Brain chemistry differs by substance, and effective treatment accounts for that.
- Stimulant addictions (cocaine, methamphetamine) respond strongly to contingency management, where clean drug screens earn tangible rewards. Because stimulants hijack the brain’s reward circuitry, providing an alternative reward source bridges the neurological gap during early recovery.
- Opioid dependencies benefit from trauma-focused work alongside behavioural therapies. Techniques like EMDR (Eye Movement Desensitization and Reprocessing) address unresolved traumatic memories that fuel continued use, since many who fall into opioid dependency were originally managing physical or emotional pain.
- Alcohol dependency responds well to the Community Reinforcement Approach, which restructures a person’s social environment to support sobriety — building rewarding alternatives that make sober living genuinely appealing.
- Cannabis use disorder has shown promising results with mindfulness-based relapse prevention (MBRP), which teaches awareness of subtle craving cues and reduces the automatic reach toward use.
What Changes as Sessions Move From Weeks Into Months?
Early sessions focus on stabilization, such as managing withdrawal effects, building a basic routine, and surviving the first few weeks without your substance of choice. Conversations center on immediate coping.
By weeks three and four, the work deepens. That surface-level history you shared during intake? Therapists now push past it. A question like “Tell me about your relationship with your father” stops being a checkbox and becomes a 45-minute excavation. The emotional material gets heavier because patients are finally stable enough to sit with discomfort without reaching for a substance to blunt it.
Around month two or three, most patients move into skill-building mode. Sessions become less about uncovering pain and more about rehearsing real responses to real triggers – what to say when a coworker offers a drink, how to leave a party without drawing attention, where to go when cravings hit at 2 a.m. Homework assignments increase. Therapists expect patients to test techniques between sessions and report back on what fell apart.
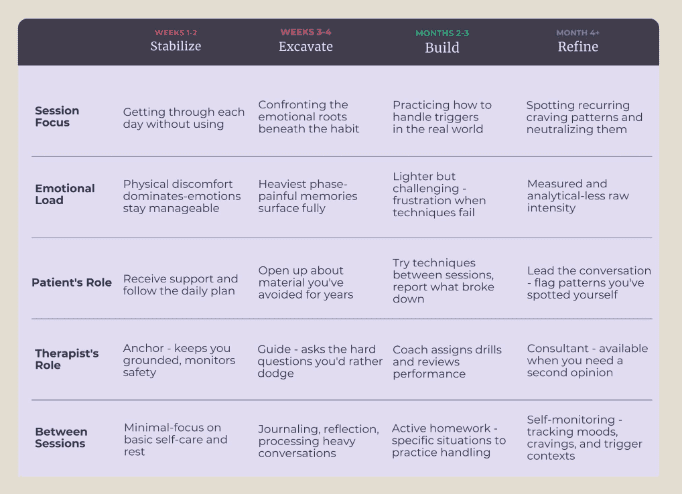
Later stages emphasize maintenance and independence. Session frequency drops – weekly becomes biweekly, then monthly. Conversations become less crisis-driven and more diagnostic. You notice a craving pattern tied to Sunday evenings? That becomes the session’s focus.
Your therapist helps you decode what Sunday triggers and builds a specific plan around it. By this point, the work feels less like treatment and more like ongoing fine-tuning.
From Stabilization to Independence
Addiction therapy is structured, deliberate work aimed at changing how a person thinks, regulates emotion, and responds to stress. Early sessions focus on stabilization and safety. Later meetings center on skill rehearsal, relapse prevention, and increasing independence. Over time, treatment becomes less about crisis control and more about strengthening the habits and decisions that support long-term recovery.















